
(Effective 1/14/2026)
Chapter 9 Overview
This chapter discusses safety planning, both Immediate Safety Intervention planning and Family Safety Planning.
Table of Contents
9.1 Outcomes of an ‘Unsafe’ Safety Assessment
9.1.1 Referral for Emergency Protective Custody
9.2 Outcomes of a ‘Safe with Plan’ Safety Assessment
9.2.1 Immediate Safety Intervention Plans
9.2.1.1 Duration of the Immediate Safety Intervention Plan (CD-263)
9.2.1.2 Monitoring of the Immediate Safety Intervention Plan (CD-263)
9.2.1.3 Background Checks and Walk-Through for a Diversion Placement with a Non-Residential Parent
9.2.1.3.1 Disqualification of a Diversion Placement with a Non-Residential Parent
9.2.1.4 Termination of an Immediate Safety Intervention Plan (CD-263)
9.2.1.5 Completing the Immediate Safety Intervention Plan (CD-263)
9.2.1.6 Safety Planning when there is a Safety Threat(s) with a Diversion Placement
9.2.2 Temporary Alternative Placement Agreement (TAPA)
9.2.2.1 Child with Relative at the Time of Report
9.2.2.2 Relative Diversion Placement Agreement Decisions
9.2.2.3 Relative Diversion Placement Background Checks
9.2.2.3.1 Disqualification of a Relative Diversion Placement
9.2.2.4 Relative Diversion Placement Requirements, Rights, and Responsibilities
9.2.2.5 Team Decision Making (TDM) Meetings
9.2.2.5.2 Facilitating TDM Meetings
9.2.2.5.3 Documenting a TDM Meeting
9.2.2.6 TAPA Monitoring Requirements
9.2.2.8 Duration and Termination of the TAPA
9.2.2.9 Intensive In-Home (IIS) Referrals
9.2.2.10 Notifying, Referring and Reporting to the Juvenile Officer
9.2.2.10.1 When the Juvenile Officer Declines a Children’s Division Referral (CD-235)
9.2.2.11 Completing the TAPA (CD-295)
9.4.1 Components of the Family Safety Planning Document (CD-267)
9.4.2 Monitoring the Family Safety Plan
9.6 Responding to Youth Presenting Signs of Suicide
9.1 Outcomes of an ‘Unsafe’ Safety Assessment
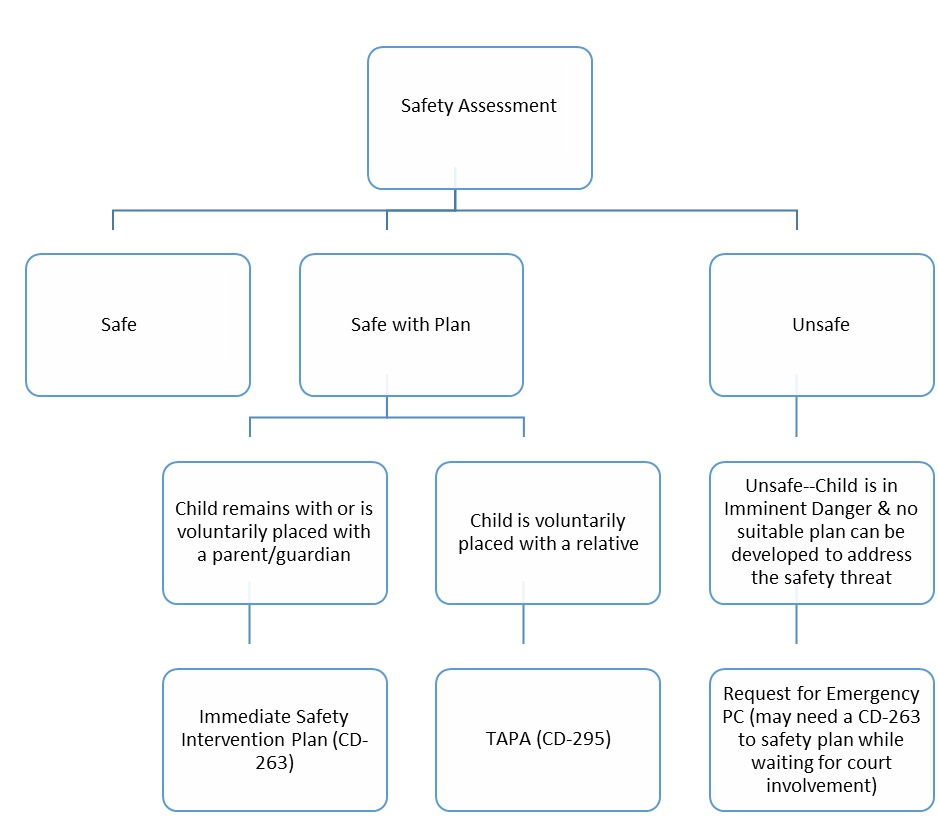
When staff determines a child is unsafe based on their assessment of the child’s safety (see Section 1, Chapter 5, Understanding and Assessing Child Safety), they must Make a referral to the Juvenile Office by submitting the Juvenile Office Referral (CD-235) with a recommendation for emergency Protective Custody if the child is determined to be in imminent danger and no suitable plan can be developed to address the safety threat(s) to the child. A copy of the SDM Safety Assessment should be sent to the Juvenile Officer with the CD-235.
9.1.1 Referral for Emergency Protective Custody
When a child is determined to be “Unsafe”, staff must assess whether the child is in imminent danger. Elements of imminent danger include:
-
- The danger must be imminent or immediate;
- A threat to life or serious physical harm, or the child has been sexually abused or is in imminent danger of sexual abuse; and
- Action needs to be taken immediately to prevent significant harm to the child, and there is not sufficient time to refer the matter to the juvenile officer and get a court order.
When the parent’s/legal guardian’s protective capacities are insufficient to control the safety threat(s) to the child and there are no viable safety interventions or supports which can be put in place to manage the safety threat(s) and the child is determined to be in imminent danger, staff should make an immediate referral to the Juvenile Office to request protective custody, either via the Emergency Request for Protective Custody (CD-234) or by completing the Juvenile Office Referral screen in FACES and submitting the Juvenile Office Referral (CD-235) to the Juvenile Office. See Section 2, Ch. 6.3, Protective Custody for further information.
It may be necessary to develop an Immediate Safety Intervention Plan (CD-263) or a Temporary Alternative Placement Agreement (TAPA), placing the child outside the home while waiting for the court process to occur, in order to keep the child safe from further harm. If the parent/legal guardian has voluntarily placed their child, but refuses to enter into an Immediate Safety Intervention Plan (CD-263) or a TAPA (CD-295) while waiting for the court to take action, staff should develop a plan with the diversion placement to identify the actions to take should the parent try to remove the child or do anything to further threaten the safety of the child.
Prior to making a referral to the juvenile court or entering into a Temporary Alternative Placement Agreement (TAPA), or as soon as possible thereafter but no later than seventy-two (72) hours, staff must consult with a professional with two years of experience in child welfare and an advanced degree in social work, or another comparable clinical human services profession. See Section 2, Ch. 6.4, Master’s Level Consultation for further information.
9.2 Outcomes of a ‘Safe with Plan’ Safety Assessment
When the Safety Assessment decision is ‘Safe with Plan’ based on staff’s assessment of the child’s safety (see Section 1, Chapter 5, Understanding and Assessing Child Safety), they must take one of the following actions:
- An Immediate Safety Intervention Plan (CD-263) is completed that allows the child to remain or be voluntarily placed with a parent/legal guardian; or,
- A Temporary Alternative Placement Agreement (CD-295) is negotiated that allows the child to be voluntarily diverted to a relative.
These steps are explained in detail below.
Note: The term ‘non-residential’ parent is used to describe a parent who does not live in the primary residence of the child and will be utilized as a diversion placement resource to protect the child from the identified safety threat(s).
Entering into either an Immediate Safety Intervention Plan or a Temporary Alternative Placement Agreement is voluntary on the part of the parents. If the Children’s Division determines that the child’s safety can only be assured by the child leaving the home, it is the parent’s choice whether to voluntarily place the child outside the home, as well as their choice on where to place the child. If the parent and the Children’s Division cannot come to an agreement on the diversion placement of the child based on the policies outlined within this section, it may be necessary to make a referral to the Juvenile Office by submitting a CD-235 if the safety of the child cannot be assured by the parent’s decisions. See Section 1, Chapter 9.3 Skillful Use of Authority.
9.2.1 Immediate Safety Intervention Plans
Pursuant to 13 CSR 35-30.020, an Immediate Safety Intervention Plan is a voluntary, time limited agreement between the Children’s Division, a child’s parent(s) and/or legal guardian(s) and any other third parties to protect a child from one or more identified, immediate threats to the child’s safety, health and welfare in the short term. The purpose of the Immediate Safety Intervention Plan is to establish and document in writing a plan to keep a child safe with the goal of preventing or eliminating the need for the child to be involuntarily removed from the child’s home and/or brought under the authority of a juvenile or family court pursuant to chapter 211 RSMo. An Immediate Safety Intervention Plan may provide for the child to remain in the child’s own home while the plan is being implemented, or temporarily reside with the non-residential parent. Any change in the residence of a child pursuant to an Immediate Safety Intervention Plan is and shall be accomplished solely pursuant to the legal authority of and voluntary consent of the child’s parent(s), legal custodian(s) or legal guardian(s). A change in the residence of a child pursuant to an Immediate Safety Intervention Plan is not intended to be and shall not be construed to be a custody order, modification of a custody order, or a placement of the child by the Children’s Division. An Immediate Safety Intervention Plan is not a custody or visitation order or a parenting plan, as such terms are otherwise defined by law. An Immediate Safety Intervention Plan does not and cannot supersede a court order governing the care, custody, control or support of a child.
If a child is determined to be unsafe, but can either remain with a parent/legal guardian (i.e. if the alleged perpetrator leaves the household) or the parent/legal guardian agrees to place the child with a non-residential parent, staff must complete the Immediate Safety Intervention Plan (CD-263). See Section 1, Chapter 9.2.1.5 Completing the Immediate Safety Intervention Plan (CD-263) for further instructions on the completion of the CD-263. Every CD-263 must be uploaded to OnBase. A copy of the CD-263 must be given to the parent/legal guardian.
When the child has been voluntarily placed outside the home with a non-residential parent and both parents agree to any diversion placement that alters any court-ordered custody arrangement, this is considered a diversion and must be entered into the Diversion Screen in FACES. Unless a TAPA has been entered into with the non-residential parent, staff do not select the TAPA box on the Diversion Screen for these types of diversions.
If it is determined that a Family-Centered Services (FCS) case should be opened to provide services, the FCS case should be opened on the parent who voluntarily placed their child outside the home. The non-residential parent and the child must be listed on the open FCS case in FACES with their whereabouts as out of the home. To further assist in monitoring the safety of the child and the parent/legal guardian’s progress with the plan developed through the FCS case, the following must also occur:
-
- Staff must have personal contact with all the children on the FCS case as appropriate, but no less than two (2) times per month. One (1) contact with each child must be a face-to-face observation of the child in the child’s diversion placement with the non-residential parent. Additional contacts with the child may occur virtually or in the community.
- At least one face-to-face home visit per month must be completed on all FCS cases with the parents.
- Follow Child Welfare Manual – Section 3 – Delivery of Services/Intact Families FCS Policy for provision of FCS services
The Children’s Division is not required to negotiate a TAPA when the child remains with a parent or is voluntarily placed with a non-residential parent. However, when the parent/legal guardian voluntarily places the child with a non-residential parent, there may be times in which a TAPA may be useful or necessary for the non-residential parent to meet the needs of the child. For example, a non-residential parent may not have established paternity, and the TAPA may be needed to meet the child’s educational, medical, mental health, etc. needs. If a TAPA is entered into with a non-residential parent, then staff must follow the procedures under TAPA, including the monitoring requirements. See Section 1, Chapter 9.2.2, Temporary Alternative Placement Agreement (TAPA).
9.2.1.1 Duration of the Immediate Safety Intervention Plan (CD-263)
Pursuant to 13 CSR 35-30.020, every CD-263 will automatically terminate without further notice ten (10) days after the date the last party signs the agreement. Each party is responsible for signing and dating the document. The CD-263 may be extended no more than ten (10) days at a time. Every extension of the Immediate Safety Intervention Plan must be done in writing and signed by all parties. The extension must specify the date on which the plan shall terminate.
In situations where the child has been maintained in the home or voluntarily placed outside the home with a non-residential parent and it is necessary to continue the CD-263 beyond ten (10) days, a supervisor consultation must be held to determine the most appropriate next steps with consideration being given to holding a Team Decision Making (TDM) meeting as described in Section 1, Chapter 9.2.2.5 Team Decision Making (TDM) Meetings, developing a TAPA as described in Section 1, Chapter 9.1.3 Safety Planning when the Child is Voluntarily Placed with a Relative—Temporary Alternative Placement Agreement, and/or opening a Family Centered Services (FCS) case. A referral to the juvenile officer should be made by submitting a CD-235 if there is no real likelihood that the threat of danger can be mitigated within a reasonable time period.
9.2.1.2 Monitoring of the Immediate Safety Intervention Plan (CD-263)
Pursuant to 13 CSR 35-30.020, the Children’s Division does not have the authority, acting on its own, to enforce the requirements of an Immediate Safety Intervention Plan. The Children’s Division retains the authority to take any action, any time and without prior notice or consultation that the Children’s Division deems in its sole discretion appropriate to protect the safety, best interests, and welfare of any child covered by an Immediate Safety Intervention Plan. This includes, but is not limited to:
-
-
- Making referrals, with or without recommendations for further action, to the Juvenile Officer;
- Making referrals to law enforcement;
- Investigating reports of child abuse or neglect and conducting family assessments;
- Sharing a copy of the Immediate Safety Intervention Plan and other relevant information with the Juvenile Officer, law enforcement, medical care providers, guardians ad litem for the child, schools and school personnel, and any other person the Children’s Division determines has a need to have the information for the care, safety and best interests of the child; and
- Negotiating a new Immediate Safety Intervention Plan or a Temporary Alternative Placement Agreement (TAPA).
-
Staff must carefully monitor all CD-263s, and these cases must be given high priority, especially when the child is particularly vulnerable or there are concerns related to the parents’ ability and/or willingness to abide by the Immediate Safety Intervention Plan. Such monitoring actions include, but are not limited to, announced and unannounced home visits by the worker or a trusted safety network member. Staff must ensure there is a plan in place to ensure the developed Immediate Safety Intervention Plan (CD-263) is being monitored regularly. It is ultimately the responsibility of the Children’s Division to monitor the Immediate Safety Intervention Plan (CD-263), and CD should therefore inform the family as to how they plan to monitor the follow-through of the plan. While other supports to the family could be utilized in the monitoring, ultimately the responsibility lies upon Children’s Division.
Pursuant to 13 CSR 35-30.020, every CD-263 will automatically terminate without further notice ten (10) days after the date the last party signs the agreement if the CD-263 is not extended. How often staff need to take some sort of action, such as phone contact with the parties, home visits, etc. to monitor the CD-263, should be determined according to the situation. However, staff must take some sort of action within the ten (10) days to monitor the Immediate Safety Intervention Plan.
If an Immediate Safety Intervention Plan is initiated, a review/update Safety Assessment must be completed every ten (10) days until the child(ren) are considered “Safe” before a report can be closed. Supervisors must staff cases with an open CD-263 at the time safety is re-assessed at the end of each ten (10) day period to determine the most appropriate next steps with consideration being given to holding a Team Decision Making (TDM) meeting as described in Section 1, Chapter 9.2.2.5 Team Decision Making (TDM) Meetings, developing a TAPA as described in Section 1, Chapter 9.2.2, Temporary Alternative Placement Agreement (TAPA), and/or opening a Family Centered Services (FCS) case. A referral to the juvenile officer should be made by submitting a CD-235 if there is no real likelihood that the threat of danger can be mitigated within a reasonable time period.
The plan for monitoring the Immediate Safety Intervention Plan is to be documented on the CD-263.
See Section 1, Chapter 9.2.1.5 Completing the Immediate Safety Intervention Plan (CD-263), for further information on monitoring the CD-263.
9.2.1.3 Background Checks and Walk Through for a Diversion Placement with a Non-Residential Parent
Pursuant to 13 CSR 35-30.020, the Children’s Division may conduct a background check of the non-residential parent and any adult member of the non-residential parent’s household, as part of its process to determine whether the non-residential parent is a suitable placement for the child.
A walk-through of the non-residential parent’s home and background check shall be conducted on the non-residential parent, as well as all adult members of the non-residential parent’s home, prior to or at the time the voluntary diversion placement is made, in order for staff to assess whether the physical environment is suitable for the child. Staff should utilize the Diversion Home and Safety Checklist (CD-293) to complete and document the walk-through.
When a parent/legal guardian voluntarily places the child with the non-residential parent, staff must take the following steps to complete a thorough background check on the non-residential parent and all adult members of their household:
-
-
- Child Abuse/Neglect (CA/N) Check: Staff must complete a child abuse and neglect check in FACES on the non-residential parent as well as all adult members of the non-residential parent’s home prior to the diversion. Staff must also conduct child abuse and neglect background checks in every state where each household member 18 years of age and older has resided for the past five (5) years, per the Adam Walsh Protection and Safety Act. Please refer to CWM 6.19.5.2, Child Abuse and Neglect Registry Out-of-State for further information on completing CA/N checks in other states. Out-of-state CA/N checks do not need to be completed prior to the parent/legal guardian’s voluntary diversion placement with the non-residential parent, but the process should be started as soon as possible.
-
- Case Net: Staff must complete a check of case net for the non-residential parent as well as all adult members of the non-residential parent’s home prior to placing the child.
-
- Sex Offender Registry: A name-based search of the sex offender registry must be completed on the non-residential parent as well as all adult members of the non-residential parent’s home prior to placing the child. Additionally, staff must complete an address-based check on the residence prior to placing the child. These checks can be completed at: https://www.mshp.dps.missouri.gov/CJ38/searchRegistry.jsp
-
9.2.1.3.1 Disqualification of a Diversion Placement with a Non-Residential Parent
Pursuant to 13 CSR 35-30.020, under no circumstances should staff agree to enter into an Immediate Safety Intervention Plan when the parent wishes to voluntarily place the child in the home of a non-resident parent where the parent or any adult member of the non-residential parent’s household has been found guilty of any offenses listed below when a child was the victim:
-
-
-
- 565.020 RSMo (murder, first degree);
- 565.021 RSMo (murder, second degree);
- 565.023 RSMo (voluntary manslaughter);
- 565.024 RSMo (involuntary manslaughter, first degree);
- 565.050 RSMo (assault, first degree);
- 566.030 RSMo (rape, first degree);
- 566.031 RSMo (rape, second degree, or 566.040 RSMo before Aug. 28, 2013);
- 566.032 RSMo (statutory rape, first degree);
- 566.060 RSMo (sodomy, first degree);
- 566.061 RSMo (sodomy, second degree, or 566.070 RSMo before Aug. 28, 2013);
- 566.062 RSMo (statutory sodomy, first degree);
- 566.064 RSMo (statutory sodomy, second degree);
- 566.067 RSMo (child molestation, first degree);
- 566.068 RSMo (child molestation, second degree);
- 566.069 RSMo (child molestation, third degree);
- 566.071 RSMo (child molestation, fourth degree);
- 566.083 RSMo (sexual misconduct involving a child);
- 566.100 RSMo (sexual abuse, first degree);
- 566.101 RSMo (sexual abuse, second degree, or 566.090 RSMo before Aug. 28, 2013);
- 566.111 RSMo (sex with an animal);
- 566.151 RSMo (enticement of a child, first degree);
- 566.203 RSMo (abusing an individual through forced labor);
- 566.206 RSMo (trafficking for the purpose of slavery, involuntary servitude, peonage, or forced labor);
- 566.209 RSMo (trafficking for the purpose of sexual exploitation);
- 566.210 RSMo (sexual trafficking of a child, first degree);
- 566.211 RSMo (sexual trafficking of a child, second degree, or 566.212 RSMo before Jan. 1, 2017);
- 566.215 RSMo (contributing to human trafficking through the misuse of documentation);
- 567.050 RSMo (promoting prostitution, first degree);
- 568.080 RSMo (child used in sexual performance, if before Jan. 1, 2017);
- 568.090 RSMo (promoting sexual performance by a child, if before Jan. 1, 2017);
- 568.020 RSMo (incest);
- 568.030 RSMo (child abandonment, first degree);
- 568.060 RSMo (abuse or neglect of a child);
- 568.065 RSMo (genital mutilation of a female child);
- 568.175 RSMo (trafficking in children);
- 573.023 RSMo (sexual exploitation of a minor);
- 573.025 RSMo (promoting child pornography, first degree);
- 573.035 RSMo (promoting child pornography, second degree);
- 573.037 RSMo (possession of child pornography);
- 573.200 RSMo (child used in sexual performance or 568.080 RSMo before Jan. 1, 2017); or,
- 573.205 RSMo (promoting sexual performance by a child or 568.090 RSMo before Jan. 1, 2017).
-
-
Pursuant to 13 CSR 35-30.020, the Children’s Division may, at its discretion, agree to enter into an Immediate Safety Intervention Plan where the parent or guardian of the child voluntarily places the child in the home of a non-residential parent where the individual or any adult member of the individual’s household has been found guilty of any other crimes against persons not listed above, substantiated or significant child abuse/neglect history, or drug and alcohol related offenses if the individual or any adult member of the individual’s household can satisfy the Children’s Division that the voluntary diversion placement is in the best interests of the child, that the individual or any adult member of the individual’s household is a fit and suitable person to temporarily care for the child, and that the household where the child will temporarily reside is safe and appropriate for the child. In making this decision, the Children’s Division may consider the following factors:
-
-
-
- Whether the individual has successfully completed the conditions of sentencing and/or probation without further incidents;
- Whether the individual has successfully completed any prescribed or required treatment;
- The duration of the time between the prior incident and the negotiation of the CD-263;
- The written advice and recommendations of professionals with knowledge of the family;
- Whether the prior incident of criminal conduct, while unlawful at the time of the incident, is no longer unlawful or proscribed at the time that the Children’s Division is considering the CD-263; and
- Any other factor or information that may be relevant to making a decision about the safety, best interests, and welfare of the child.
-
-
If the parent/legal guardian wishes to voluntarily place the child with a non-residential parent, including any members of the non-residential parent’s household, who has been found guilty of any other crimes against persons not listed above, has a substantiated or significant child abuse/neglect history, or has drug and alcohol related offenses AND the Children’s Division determines this voluntary diversion placement to be in the safety, best interest, and welfare of the child, approval must be obtained through supervisory channels. In emergency or after-hours situations, this approval may be given by the supervisor and/or Circuit Manager. Staff should then follow up with obtaining approval from the Regional Director, or their designee, the following business day.
If the parent/legal guardian and the Children’s Division are unable to reach an agreement regarding the immediate diversion placement of the child with a parent when they cannot be safely maintained in the home, staff should discuss the possibility of placing the child with a relative and entering into a Temporary Alternative Placement Agreement (TAPA) or making an immediate referral to the juvenile officer by submitting a CD-235.
9.2.1.4 Termination of an Immediate Safety Intervention Plan (CD-263)
Pursuant to 13 CSR 35-30.020, under no circumstances may a Child Abuse/Neglect (CA/N) report be closed with an open CD-263 unless the case has been referred to ongoing case management. Staff must continue to monitor the CD-263 as described above until the safety threat(s) requiring the CD-263 are eliminated.
The Children’s Division should not terminate its involvement with the family until the non-residential parent can establish or modify custody or obtain an order of child protection as long as there is a need for a CD-263 due to an immediate safety threat(s) to the child. For orders of child protection, staff should ensure a permanent, not just a temporary, order has been granted prior to case closure.
If the safety threat(s) that caused the child to be voluntarily placed with a non-residential parent cannot be eliminated prior to the CA/N report conclusion timeframe, staff should consider developing a TAPA and/or making a referral to the juvenile officer by submitting a CD-235. If there is a need to extend the CD-263 because the safety threat(s) that caused the child to be voluntarily placed with a non-residential parent has not been eliminated, staff should also consider opening a Family Centered Services (FCS) case prior to the conclusion of the CA/N report to monitor the family’s progress and implement any safety-related services necessary to eliminate the immediate safety threat.
Pursuant to 13 CSR 35-30.020, Immediate Safety Intervention Plans are voluntary. Any party to the CD-263 may terminate their participation in the Immediate Safety Intervention Plan at any time with reasonable notice to the other participants. Any party wishing to terminate their participation shall notify the Children’s Division, preferably in writing. If a family refuses to participate in the CD-263, it may be necessary to make a referral to the Juvenile Court by submitting a CD-235 if the safety of the child cannot be assured.
The Children’s Division retains the authority to refer the case to the juvenile officer with a recommendation for further action while an Immediate Safety Intervention Plan is in place. If at any time during the Immediate Safety Intervention Plan it is determined that the goals are not being accomplished within the time period specified, and the safety, best interest, and welfare of the child cannot be assured if returned home, staff should refer the family to the juvenile officer.
Staff must clearly document in the case record when the CD-263 is terminated and the rationale for determining the child to be safe.
9.2.1.5 Completing the Immediate Safety Intervention Plan (CD-263)
Pursuant to 13 CSR 35-30.020, each Immediate Safety Intervention Plan (CD-263) will be reduced to writing and signed by the parties to the plan. It will:
-
-
- Identify the danger or immediate safety threat(s) to the child;
- Identify the services that the Children’s Division may offer to address the identified safety threat(s) to the child;
- Identify the specific actions that the child’s parent/legal guardian will take to address the identified safety threat(s) to the child, and specify the time frames during which those actions will be completed;
- Identify any other people or agencies that are willing and available to support the child and the parent/legal guardian in the implementation of the Immediate Safety Intervention Plan (CD-263), and identify what actions they may take to implement the plan;
- Include a statement that the parent/legal guardian agrees to the Immediate Safety Intervention Plan (CD-263), that they will participate in good faith with the services offered by the Children’s Division, that they will cooperate with the Children’s Division and that they will implement the requirements of the Immediate Safety Intervention Plan (CD-263);
- Specify the date on which the Immediate Safety Intervention Plan (CD-263) will terminate;
- Contain any other provisions that the parties may deem appropriate; and
- Include a plan for monitoring the effectiveness of the Immediate Safety Intervention Plan (CD-263).
-
The Immediate Safety Intervention Plan (CD-263) must be completed at any point during Children’s Division’s casework with families in which there are immediate threats to child safety. The CD-263 is not to be used as a questionnaire, but rather as a tool to developing an agreed upon plan along with the family and their support network in order to mitigate any immediate safety threats.
The CD-263 should be seen as a flexible agreement dependent on the effectiveness in controlling the safety threat(s) to the child. They should be evaluated, readjusted, or modified as needed.
What immediate safety threat(s) to the child(ren) exist?
A safety threat is defined as a behavior, emotion, motive, perception, or capacity of a person who has access to the child that is out of control, imminent, and likely to have severe effects on a vulnerable child. When identifying safety threat(s), they need to be child specific. Safety threats to a child are evident when a child is vulnerable to a particular situation and the parent/legal guardian does not have the protective capacities to resolve the threat.
Staff should document what safety threat was identified from the SDM Safety Assessment on the CD-263.
Example: A report is received regarding a parent who was unresponsive due to a drug overdose. A three-year-old child was found in the home when first responders arrived on the scene. The safety threat would be that a parent’s substance use impairs their ability to supervise, protect, or create a safe environment for the child, and the child is likely to be harmed without intervention. This would be identified as Safety Threat 5.
What are the child’s vulnerabilities to the safety threat(s), and what are the concerns with the parent(s)/caretaker(s) protective capacities?
Vulnerabilities of a child are a significant factor in evaluating the safety and imminency of the identified safety threat(s). Child vulnerabilities are the degree to which a child is susceptible to threats to his or her safety and the degree to which a child is capable of protecting him/herself against those threats. Things that contribute to child vulnerabilities are age, developmental level and mental capacities, physical disabilities and illness, behaviors, ability to communicate, isolation/visibility, ability to meet basic needs, access to perpetrator(s), and child’s relationship to perpetrator(s).
Example: With the above safety threat example in mind, there would be a great difference in the vulnerabilities of an infant and those of a sixteen-year-old. An infant would not have the ability to provide for their own basic needs if their parent were under the influence of methamphetamines, as an infant is entirely dependent on others for their care. On the other hand, a sixteen-year-old would potentially have the ability to protect themselves, as long as the teenager was of typical development, and/or would likely have the ability to access a safety network resource if their parent was under the influence of a mind-altering substance.
The protective capacities of a parent/legal guardian are another vital element to consider when evaluating safety. Caregiver protective capacities are personal, behavioral, cognitive, and emotional characteristics that are directly associated with child protection. There are several things that can impact the protective capacities of a parent/legal guardian, including mental capabilities, physical health, access to resources, relationship to the perpetrator(s), behavioral history, age, and substance misuse.
Example: If a parent/legal guardian was verified to be using methamphetamines while parenting their infant, their protective capacities are negatively impacted as they would not have the cognitive or behavioral ability to readily provide for the basic needs of their infant while under the influence.
What actions have the parent/legal guardian taken in the past to keep the child safe when the safety threat(s) have occurred? What supports have been utilized in the past (or presently) to keep the child(ren) safe?
By exploring previous safety threats and what the parent/legal guardian did in the past to keep the child safe, strengths within the family are identified. Similarly, once past and/or present supports to keep the child safe are explored, possible support networks (either formal or informal supports) are identified that can assist with the current Immediate Safety Intervention Plan (CD-263). By expanding on strengths within the parental protective capacities and identifying natural supports within each family, staff are more easily able to assist the family in developing realistic plans that are specific to their family, making follow-through more likely. It also allows the parent/legal guardian an opportunity to feel actively involved in the plans for their family, instead of being directed on what to do from an outside agency.
To address the ongoing safety threat(s), we will implement the following plan:
When developing the Immediate Safety Intervention Plan (CD-263), staff should take into account all of the above elements, including the immediacy of the safety threat(s), child vulnerabilities, parent/legal guardian’s protective capacities, and actions/supports that have been successful in keeping the child safe in the past. The plan should be individually specific, behaviorally specific, realistic, and time-limited.
When developing an Immediate Safety Intervention Plan (CD-263), the Children’s Division may consider the following factors and considerations:
-
-
- Utilize the family’s own resources first by focusing on existing strengths within the family and their network;
- Utilize the least intrusive interventions that will control or manage the safety threat(s);
- Involve the alleged perpetrator to the extent possible and appropriate without compromising the safety of the child. The nature of their relationship to the child and family should be taken into consideration in deciding if and how the alleged perpetrator’s involvement will happen;
- Assess the reliability of sources or providers of the action or supports. (Informal: friend, relative, neighbor or Formal: school, agency, assistance programs…do they know they are included in the plan?);
- Develop interventions to accommodate time elements (for example, weekends and holidays may require different actions than daytime hours during the week, etc.);
- Develop overlapping interventions to accommodate scheduling or to address times when the safety concern is active;
- Take into consideration the tradeoffs the family may have to make in order to implement the Immediate Safety Intervention Plan (CD-263);
- Be conscious not to create further trauma to the family; and
- Meet the following criteria:
- Immediately available – can be deployed right now and in a sufficient way;
- Action-oriented – steps/agreements that are active and focused with respect to safety concerns; not change, service, or treatment reliant;
- Flexible access – safety resources that are located in acceptable proximity and can be called upon for immediate response;
- Have immediate impact – actions or resources that do what they are supposed to do as they are delivered and achieve the objective…keep children safe; and
- No promissory commitments – Safety Interventions will never rely on parental promises to stop the threatening behavior; for example, “I will stop drinking” or “I will always supervise the child”. Safety interventions should provide an alternative action or a third party to assist in controlling the actualization of the danger statement.
-
How will this Immediate Safety Intervention Plan be monitored?
It must be clear to everyone involved in the safety intervention what their responsibilities are in relation to the intervention, what the plan for monitoring is, and that monitoring includes a focus on:
-
-
- Successful use of the plan/intervention;
- Effectiveness of the Immediate Safety Intervention Plan (CD-263) and the need for adjustment and modifications;
- Ongoing assessment of the identified safety threats;
- The emergence of new threats or escalating threats; and
- Conditions are either resolved or no longer meet the safety threshold criteria.
-
In developing a plan for monitoring an Immediate Safety Intervention Plan (CD-263), the worker must consider the following:
-
-
- As long as conditions are unsafe, safety interventions must be in place;
- When there is no longer a safety threat, the need for an Immediate Safety Intervention Plan (CD-263) is resolved; and
- Immediate Safety Intervention Plans (CD-263) must be monitored and may need to be adjusted or modified to ensure the interventions are effectively controlling the threat of danger.
-
The plan for monitoring the Immediate Safety Intervention Plan must include:
-
-
- Who will be used to monitor the plan?;
- Date/time of initial follow-up? Initial follow-up should be within a day or two. Staff should consider whether there is a need to complete any follow-up during non-business hours. Staff, in conjunction with their supervisor, should develop a plan to follow up with the family if it is necessary during non-business hours. Announced and unannounced home visits by the worker or trusted safety network member may be necessary to ensure the Immediate Safety Intervention Plan (CD-263) is being adhered to;
- Frequency of monitoring action. Pursuant to 13 CSR 35-30.020, every CD-263 will automatically terminate without further notice ten (10) days after the date the last party signs the agreement. How often staff need to take some sort of action, such as phone contact with the parties, home visits, etc., should be determined according to the situation. However, staff must take some sort of action within the ten (10) days to monitor the Immediate Safety Intervention Plan (CD-263);
- Monitoring Action – Direct contact with the caregiver, protective resource or child by the worker or a safety network member. If the worker is not the one monitoring the plan directly, the worker should be updated by the safety network member according to the specified plan; and
- An explanation of how and how frequently any safety network member will assist in monitoring the Immediate Safety Intervention Plan and how they will communicate with the Children’s Division;
-
Monitoring includes:
-
-
- Verification of implementation;
- Effectiveness of intervention;
- Credibility, availability, and accessibility of the safety network;
- Flexibility of safety interventions to adjust for control of the safety threat;
- Understanding from the participants that plans must be modified if the Immediate Safety Intervention Plan (CD-263) is no longer effective in controlling the safety threat; and
- Understanding that the Immediate Safety Intervention Plan (CD-263) is short-term.
-
What safety-related resources/support services are currently in place or still need to be referred to assist with the behavioral changes needed to resolve the threat(s) of safety to the child? What services will the Children’s Division offer to the family? What supports have been utilized in the past that can be utilized during the Immediate Safety Intervention Plan to eliminate the safety threat(s)?
This section of the CD-263 is separated from the actual plan for safety, as an Immediate Safety Intervention Plan should not be reliant on services to make immediate behavioral change.
In this section of the Immediate Safety Intervention Plan (CD-263), staff shall identify all safety-related services, service providers, and specific resources being offered to any and all parties involved in the CD-263, as well as what safety-related services and supports the family still needs to be connected with in an effort to prevent the removal of the child. These can be direct services provided by the Children’s Division as well as any other services from community agencies that have been offered to the family to assist with the success of the Immediate Safety Intervention Plan (CD-263) and to reduce the risk of future CA/N. Safety-related services are appropriate services that are provided to or arranged for the family with the goal of ensuring child safety. For example, if there are safety concerns related to the parent’s ability to manage child-specific needs, Intensive In-Home Services (IIS) can be an appropriate safety-related services.
Staff should be sure to include timeframes for each service/resource and how the implementation of such service(s)/resource(s) will assist with the successful termination of the CD-263.
When staff determine safety-related services are needed during a CA/N report staff should clearly articulate and document the safety concern to include areas of need such as, but not limited to: basic needs, living conditions, the family’s support system, health, mental health, educational concerns, and help address the needs through community resources and/or the family’s safety network.
What steps should the family and/or safety network members take in the event that this Immediate Safety Intervention Plan is violated? Provide the name(s) and contact information for all members of the family support network as well as all individuals who must be immediately notified if this Safety Intervention Plan is violated or there are concerns for the safety of the child(ren) involved in this plan:
The Immediate Safety Intervention Plan (CD-263) must include an action step(s) for notification if the plan is violated or concerns arise regarding the safety of the child. This action step(s) should be developed so that all those involved in the Immediate Safety Intervention Plan (including formal/informal family supports, collaborative team members, service providers, etc.) will know what to do in the event the plan is violated. This should include contact information for all those who must be immediately notified if the plan is violated or concerns arise regarding the safety of the child.
Once the CD-263 is developed, the worker should make sure the family and any safety network members actively involved in the plan have a copy. The worker can take a picture of the plan for the record and provide the family with a paper copy. A copy must be retained and uploaded to OnBase.
The parent/legal guardian shall cooperate in good faith with the Children’s Division to implement the Immediate Safety Intervention plan:
Prior to members involved in the Immediate Safety Intervention Plan (CD-263) signing the document, it is the responsibility of Children’s Division staff to ensure all signing members read and understand their responsibilities, including the following:
-
-
- Making the child available to meet with the Children’s Division or its contractors/representatives in the State of Missouri in person, virtually, or by other means of communication upon request to enable the Children’s Division to ensure the Immediate Safety Intervention Plan (CD-263) is being implemented and the child is safe and well cared for throughout the duration of the plan.
- Allowing the Children’s Division or its contractors/representatives to inspect the home at reasonable times (announced and unannounced) to ensure the Immediate Safety Intervention Plan (CD-263) is being implemented.
- Executing any consents and/or authorizations to release information to the Children’s Division and/or to or from third parties the Children’s Division determines necessary to obtain information to develop and/or monitor the implementation of the Immediate Safety Intervention Plan (CD-263). This includes, but is not limited to: health care providers, schools, and other professionals providing services to the child or other parties.
- Keeping the Children’s Division informed of the parent/legal guardian’s current residence address, mailing address, telephone number, email address, and any other contact information, as well as changes in the residence and contact information for the child.
- Promptly notify the Children’s Division of any change in circumstances that may impact the care of the child and/or the implementation of the Immediate Safety Intervention Plan (CD-263).
-
9.2.1.6 Safety Planning when there is a Safety Threat(s) with a Diversion Placement
Staff continuously assesses child safety at every contact with the child, the family, and any placement a child may be in. If a child is in a diversion placement, either with a non-residential parent or a relative AND staff assess that the child is unsafe in the home of the diversion placement, staff must develop a plan to address the safety threat(s). If it is determined that the child may remain in the home of the diversion placement with an appropriate plan in place, staff must develop an Immediate Safety Intervention Plan (CD-263). The child’s parent/legal guardian must agree to the terms of the CD-263 and allow the child to remain in the home of the diversion placement. If it is determined that the child cannot safely remain in the home of the diversion placement AND it remains unsafe for the child to return to the home of the parent/legal guardian, consideration must first be given to developing a Temporary Alternative Placement Agreement (TAPA) as described in Section 1, Ch. 9.2.2 Temporary Alternative Placement Agreement (TAPA). If a TAPA cannot be negotiated in these circumstances, staff should make a referral to the juvenile officer by submitting a CD-235 as soon as possible.
9.2.2 Temporary Alternative Placement Agreement (TAPA)
NOTE ON THE DEFINITION OF A RELATIVE: Pursuant to Section 210.565 and 13 CSR 35-30.020, the term ‘relative’ shall mean a grandparent or any other person related to another by blood or affinity or a person who is not so related to the child but has a close relationship with the child or the child’s family. The status of a grandparent shall not be affected by the death or dissolution of the marriage of a son or daughter.
If a child is determined to be unsafe, there may be times when they can be temporarily placed outside of the home with a relative to allow for time to reduce or eliminate the safety threat(s) to the child and to attempt to prevent the child from being involuntarily removed from their parent/legal guardian. These voluntary placements are termed “diversion placements”. All diversions must be entered into the Diversion Screen in FACES. Staff must select the TAPA box on the Diversion Screen for all diversions that resulted in the negotiation of a TAPA and complete additional TAPA specific questions.
Pursuant to Section 210.123, RSMo and 13 CSR 35-30.030, a TAPA is a voluntary agreement between the Children’s Division, a relative of the child, and the parent or guardian of the child to provide a temporary out of home placement for a child if the parent or guardian is temporarily unable to provide care or support for the child and the child is not in imminent danger of death or serious bodily injury, or being sexually abused such that the Children’s Division determines that a referral to the juvenile officer by submitting a CD-235 with a recommendation to file a petition or to remove the child is not appropriate.
A TAPA requires the agreement and signature of the following parties:
-
- The parent/legal guardian;
- The relative; and
- The Children’s Division
If the parties are unable to reach an agreement regarding the terms of the TAPA, staff must make a referral to the juvenile officer by submitting a CD-235 as soon as possible, but no later than three (3) business days from the date of the diversion placement.
The parent/legal guardian who is considered the party to the TAPA is generally considered to be the parent/legal guardian with whom the safety threat(s) exist and from whom the child is being diverted. If that parent/legal guardian is unavailable to be a party to the TAPA, consideration should be given to entering into a TAPA with the non-residential parent if that parent is not an appropriate diversion placement as discussed in Section 1, Ch. 9.2.1 Immediate Safety Intervention Plans. If a non-residential parent does not agree to the terms of the TAPA developed with the parent/legal guardian, staff should make a referral to the Division of Legal Services for assistance in determining the most appropriate next steps.
While the child is not explicitly a party to the TAPA pursuant to Section 210.123, RSMo, staff should explain to the child, in an age and developmentally appropriate manner, that concern exists for the safety and wellbeing of the child and family and that other persons need to become involved to help the family. As a party to the TAPA, the Children’s Division does not have to enter into a TAPA if the child does not agree to the terms. Staff should give consideration to the child’s wishes based on an assessment of the child’s best interests. If the child does not agree to the terms of the TAPA, consideration should be given to including them in the initial Team Decision Making (TDM) meeting as discussed in Section 1, Ch. 9.2.2.5.1, Initial TDM Meeting to work through the concerns of the child and to attempt to develop an appropriate plan to address the safety threat(s) with all parties, including the child when age and developmentally appropriate.
Pursuant to Section 210.123, RSMo, the Children’s Division may only enter into a TAPA if:
-
- The child cannot remain safely in the home of the child’s parent or legal guardian;
- It is not apparent that the child is otherwise in imminent danger of death, serious physical injury, or being sexually abused such that an immediate referral to the juvenile officer by submitting a CD-235 with a recommendation to remove the child and initiate juvenile court proceedings is appropriate. (See Section 1, Chapter 9.1.1, Referral for Emergency Protective Custody);
- There is a relative who is ready, willing, and able to provide safe care for the child on a temporary basis;
- The Children’s Division has reasonably available services for the child and family to support and supervise the implementation of the agreement;
- The child’s parent or legal guardian voluntarily enters into the agreement; and,
- The child’s parent or legal guardian executes all necessary documents and consents to implement the agreement.
Once staff complete their Safety Assessment and determine the child to be unsafe, they must immediately take action to develop a plan to address the safety threat(s). If it is determined the child can be safely diverted to a relative and a TAPA is therefore necessary, staff must complete the Temporary Alternative Placement Agreement (CD-295) as soon as possible, but no later than three (3) business days from the date the diversion placement was made and shall be signed by the parent/guardian, the relative, and appropriate Children’s Division staff. Staff must begin the CD-295 at the time of the diversion placement, but do not have to have the CD-295 finalized at that time. For example, staff may develop a rough draft of the CD-295 with the family at the time of the diversion, but may choose to utilize the initial TDM meeting to finalize the CD-295 once more information is gathered and the TAPA has been fully discussed with the relative. NOTE: Pursuant to Section 210.123 RSMo, the CD-295 must be reduced to writing within three business days of the diversion and is not a final agreement until the parent/legal guardian, relative, and the Children’s Division have signed it.
If the parent/legal guardian voluntarily places the children with the same relative, siblings may be included under one CD-295. Staff must make sure to assess and identify each child’s specific vulnerabilities to the safety threat(s) and should identify action steps/safety interventions for each child depending on their individual needs. The CD-295 should be specific to the relative diversion placement. Therefore, if siblings will not be staying together, separate CD-295s should be completed.
NOTE: In the event a TAPA cannot be negotiated, staff may need to complete an Immediate Safety Intervention Plan (CD-263) to attempt to address the safety threat(s). However, if a CD-263 is utilized to address the safety threat(s) because the parties do not agree to the conditions of a TAPA, staff must make a referral to the juvenile officer, via the CD-235.
Example: Staff respond to an investigation and assess the child to be unsafe; there is no other parent to divert the child to (because CD first has to explore whether the child can safely remain with or be placed with a parent). The parent identifies a relative they are willing to temporarily place the child with, but the parent refuses to participate in an FCS case. In this scenario, staff could do a CD-263 with all parties agreeing to the diversion with the relative, but CD must make a referral to the juvenile officer because the parent, a party, did not agree to a TAPA. In this scenario, if the parent also refused to enter into a CD-263, the staff must make an immediate referral to the juvenile officer.
Every CD-295 must be uploaded to OnBase. A copy of the CD-295 is to be provided to the parent/legal guardian and the relative, as well as the juvenile officer immediately upon completion, but no later than three (3) business days from the date of the diversion placement. See Section 1, Ch. 9.1.3.11, Completing the TAPA (CD-295) for further information.
Prior to entering into a Temporary Alternative Placement Agreement (TAPA), or as soon as possible thereafter but no later than seventy-two (72) hours, staff must consult with a professional with two years of experience in child welfare and an advanced degree in social work, or another comparable clinical human services profession. See Section 2, Ch. 6.4, Master’s Level Consultation for further information.
9.2.2.1 Child with Relative at the time of report
There may be instances where the Children’s Division receives a report on a child that is already residing with a relative. After initial safety of the child is assured, the home will be assessed on the appropriateness of the child continuing to reside in the relative’s home. If there are no concerns with the child remaining with the relative, the Children’s Division does not have to enter into a TAPA. However, the Children’s Division and relative may find instances where the placement of the child is appropriate, but the relative needs assistance with services such as getting educational, medical, and mental health authorization(s) for the child. If the Children’s Division, the parent, and the relative agree and find it appropriate, a TAPA may be developed to assist with services or to obtain a power of attorney, an affidavit for relative caretaker, legal guardianship, an order of child protection or legal custody. If the parent cannot be located or does not agree to the terms of a TAPA and the TAPA is necessary to meet the needs of the child, staff must make a referral to the juvenile officer by submitting a CD-235. Termination of the TAPA may be executed once the services have been provided or otherwise no longer needed to assist the child and the relative.
9.2.2.2 Relative Diversion Placement Agreement Decisions
When a child is unable to safely remain in their home with their parent/guardian, consideration should first be given to whether the immediate safety threat(s) could be mitigated if the parent chose to place the child with a non-residential parent. The Children’s Division is not required to negotiate a TAPA when the child remains with a parent or is voluntarily placed with a non-residential parent. However, when the parent/legal guardian voluntarily places the child with a non-residential parent, there may be times in which a TAPA may be useful or necessary for the non-residential parent to meet the needs of the child. For example, a non-residential parent may not have established paternity and the TAPA may be needed to meet the child’s educational, medical, mental health, etc. needs. If a TAPA is entered into with a non-residential parent, then staff must follow the procedures under TAPA, including the monitoring requirements.
Pursuant to 13 CSR 35-30.030, the Children’s Division will give first consideration to entering into a TAPA with the child’s other parent when the child and the child’s parents do not reside in the same household. Pursuant to 13 CSR 35-30.030, if it is determined that the other parent is not a suitable placement the Children’s Division will give second consideration to enter into a TAPA with the child’s grandparent. If the Children’s Division cannot agree to enter into an Immediate Safety Intervention Plan in which the parent/legal guardian voluntarily places the child with the other parent, staff should then work with the family in an attempt to identify a fit and willing relative that all parties can agree on to provide a safe temporary alternative placement for the child. However, ultimately it is the parent’s choice with whom to place their child. If the Children’s Division cannot agree with the parent’s choice, staff must make a referral to the juvenile officer by submitting a CD-235.
Pursuant to Section 210.123, RSMo and 13 CSR 35-30.030, the relative must be a resident of Missouri and both the child and the relative are required to reside in Missouri for the duration of the TAPA. The child may reside out of state only if the child requires medical treatment in another state that is not reasonably available within Missouri. Because of these stipulations, if the parent chooses to voluntarily place the child with a relative out of state the Children’s Division may not enter into a TAPA and must refer the family to the juvenile officer via the CD-235.
Pursuant to 13 CSR 35-30.030, in making the decision to enter into a TAPA and deciding what services the Children’s Division may be able to offer to assist the parties in implementing the plan, the Children’s Division may consider and balance:
-
-
- The wishes of the parent and relative;
- The wishes of the child;
- The needs of the child for safe, frequent, continuing, and meaningful relationship between the child and the child’s parent;
- The ability and willingness of the parent and the relative to actively perform their functions for the needs of the child;
- The interaction and interrelationship of the child with the child’s parent, siblings, grandparents, the relative, and any other person who may significantly affect the child’s best interests;
- The child’s adjustment to their home, school, and community;
- The mental and physical health of all individuals involved;
- Any history of abuse or neglect of any individual involved;
- Any history of domestic violence;
- Any special needs of the child, the child’s level of care, and the needs of the child’s parent, and the relative;
- The financial and personal resources available to the parent and the relative to care for the child and implement the plan set out in the TAPA. This may include whether the child, the child’s parent, and the relative may be eligible for benefits and services through other governmental and private organizations;
- The resources and services available to the Children’s Division, including the availability of appropriated funds for the provision of resources and services;
- The educational needs of the child;
- The willingness and ability of the parent, the relative, the child, and the relative’s household members to work with the Children’s Division and each other to cooperatively develop and implement the TAPA;
- Any history of criminal activity of any individual involved that may pose a safety risk to the child or impact the ability or willingness of any individual to implement the TAPA;
- Any current or past history of conduct that may indicate substance use disorder by the child, the parent, the relative, other members of the relative’s household, or other persons;
- The number of children in the home or being placed in the home; and
- Any other facts, information, or considerations the Children’s Division deems relevant to its decision.
-
Once the parent/legal guardian identifies a relative they wish to voluntarily place the child with, staff will immediately contact the relative to inquire if they are willing to take the child and work with the Children’s Division to develop and monitor the TAPA. The relative provider, and all adult members of the relative’s household, must also agree to undergo background checks before the diversion placement of the child is to be made.
9.2.2.3 Relative Diversion Placement Background Checks
Pursuant to 13 CSR 35-30.030, the Children’s Division may conduct a background check of the relative, and any adult member of the relative’s household as part of its process to determine whether the relative is a suitable temporary placement for the child. The relative, and other adult household members, shall execute any consents or other documents necessary to complete any background checks. If the relative, or any adult member of the relative’s household, declines to complete the background check process, then the Children’s Division may not enter into a TAPA.
A walk-through of the relative’s home and background check shall be conducted on the relative, as well as all adult members of the relative’s home before determining, prior to or at the time the voluntary diversion placement is made in order for staff to assess whether the physical environment is suitable for the child. Staff should utilize the Diversion Home and Safety Checklist (CD-293) to complete and document the walk-through.
Background checks must include the following:
-
-
- Child Abuse/Neglect (CA/N) Check: Staff must complete a child abuse and neglect check in FACES on the relative and all adult household members residing in the relative’s home prior to the diversion. Staff must also conduct child abuse and neglect background checks in every state where each household member 18 years of age and older has resided for the past five (5) years, per Adam Walsh Protection and Safety Act. Please refer to CWM 6.19.5.2, Child Abuse and Neglect Registry Out-of-State for further information on completing CA/N checks in other states. Out of state CA/N checks do not need to be completed prior to the parent/legal guardian’s voluntary diversion placement with the relative, but the process should be started as soon as possible.
-
- Case Net: Staff must complete a check of case net for the relative and every adult member of the relative’s household prior to placing the child.
-
- Sex Offender Registry: A name-based search of the sex offender registry must be completed on the relative and all adult household members in the relative’s home prior to placing the child. Additionally, staff must complete an address-based check on the relative’s residence prior to placing the child. These checks can be completed at: https://www.mshp.dps.missouri.gov/CJ38/searchRegistry.jsp
-
- Family Safe Care Registry: Upon entering into the TAPA, the relative and each household member 18 years of age and older must register with the Family Care Safety Registry (FCSR). The FCSR is maintained by the Department of Health and Senior Services (DHSS). Staff will provide the applicant with instructions regarding the process for each adult in the household to register with the FCSR on the Internet. This registration must be completed as quickly as possible. Staff may assist the applicant with the online registration. Refer to CWM 6.9.3 Family Care Safety Registry for further information.
-
NOTE: Staff should inform the provider to check the ‘Foster Parent/Family Member of Foster Parent’ box on the registration form to avoid having to pay registration fees.
Staff may telephone the FCSR at 1-866-422-6872 to make a background screening request. Generally, information will be available within two weeks. An oral report will be given at the time of the call and will be followed with a written report to both the requestor and the registrant within 48 hours. Staff may also access the FCSR online as outlined in CWM 6.19.3 Family Care Safety Registry.
9.2.2.3.1 Disqualification of a Relative Diversion Placement
Pursuant to 13 CSR 35-30.030, under no circumstances should staff agree to enter into a TAPA when the parent wishes to voluntarily place the child in the home of a relative where the relative or any adult member of the relative’s household has been found guilty of any offenses listed below when a child was the victim:
-
-
-
- 565.020 RSMo (murder, first degree);
- 565.021 RSMo (murder, second degree);
- 565.023 RSMo (voluntary manslaughter);
- 565.024 RSMo (involuntary manslaughter, first degree);
- 565.050 RSMo (assault, first degree);
- 566.030 RSMo (rape, first degree);
- 566.031 RSMo (rape, second degree, or 566.040 RSMo before Aug. 28, 2013);
- 566.032 RSMo (statutory rape, first degree);
- 566.060 RSMo (sodomy, first degree);
- 566.061 RSMo (sodomy, second degree, or 566.070 RSMo before Aug. 28, 2013);
- 566.062 RSMo (statutory sodomy, first degree);
- 566.064 RSMo (statutory sodomy, second degree);
- 566.067 RSMo (child molestation, first degree);
- 566.068 RSMo (child molestation, second degree);
- 566.069 RSMo (child molestation, third degree);
- 566.071 RSMo (child molestation, fourth degree);
- 566.083 RSMo (sexual misconduct involving a child);
- 566.100 RSMo (sexual abuse, first degree);
- 566.101 RSMo (sexual abuse, second degree, or 566.090 RSMo before Aug. 28, 2013);
- 566.111 RSMo (sex with an animal);
- 566.151 RSMo (enticement of a child, first degree);
- 566.203 RSMo (abusing an individual through forced labor);
- 566.206 RSMo (trafficking for the purpose of slavery, involuntary servitude, peonage, or forced labor);
- 566.209 RSMo (trafficking for the purpose of sexual exploitation);
- 566.210 RSMo (sexual trafficking of a child, first degree);
- 566.211 RSMo (sexual trafficking of a child, second degree, or 566.212 RSMo before Jan. 1, 2017);
- 566.215 RSMo (contributing to human trafficking through the misuse of documentation);
- 567.050 RSMo (promoting prostitution, first degree);
- 568.080 RSMo (child used in sexual performance, if before Jan. 1, 2017);
- 568.090 RSMo (promoting sexual performance by a child, if before Jan. 1, 2017);
- 568.020 RSMo (incest);
- 568.030 RSMo (child abandonment, first degree);
- 568.060 RSMo (abuse or neglect of a child);
- 568.065 RSMo (genital mutilation of a female child);
- 568.175 RSMo (trafficking in children);
- 573.023 RSMo (sexual exploitation of a minor);
- 573.025 RSMo (promoting child pornography, first degree);
- 573.035 RSMo (promoting child pornography, second degree);
- 573.037 RSMo (possession of child pornography);
- 573.200 RSMo (child used in sexual performance or 568.080 RSMo before Jan. 1, 2017); or,
- 573.205 RSMo (promoting sexual performance by a child or 568.090 RSMo before Jan. 1, 2017).
-
-
Pursuant to 13 CSR 35-30.030, the Children’s Division may, at its discretion, agree to enter into a TAPA where the parent or guardian of the child places the child in the home of a relative where the individual or any adult member of the individual’s household has been found guilty of any other crimes against persons not listed above, substantiated or significant child abuse/neglect history, or drug and alcohol related offenses if the individual or any adult member of the individual’s household can satisfy the Children’s Division that the diversion placement is in the best interests of the child, that the individual or any adult member of the individual’s household is a fit and suitable person to temporarily care for the child, and that the household where the child will temporarily reside is safe and appropriate for the child. In making this decision the Children’s Division may consider the following factors:
-
-
-
- Whether the individual has successfully completed the conditions of sentencing and/or probation without further incidents;
- Whether the individual has successfully completed any prescribed or required treatment;
- The duration of the time between the prior incident and the negotiation of the TAPA;
- The written advice and recommendations of professionals with knowledge of the family;
- Whether the prior incident of criminal conduct, while unlawful at the time of the incident, is no longer unlawful or proscribed at the time that the Children’s Division is considering the TAPA; and
- Any other factor or information that may be relevant to making a decision about the safety, best interests, and welfare of the child.
-
-
If the parent/legal guardian wishes to voluntarily place the child with a relative, including any members of the relative’s household, who has been found guilty of any other crimes against persons not listed above, has a substantiated or significant child abuse/neglect history, or has drug and alcohol related offenses AND the Children’s Division determines this diversion placement to be in the safety, best interest, and welfare of the child, approval must be obtained through supervisory channels. In emergency or after-hours situations, this approval may be given by the supervisor and/or Circuit Manager. Staff should then follow up with obtaining approval from the Regional Director, or their designee, the following business day.
9.2.2.4 Relative Diversion Placement Requirements, Rights, and Responsibilities
Pursuant to Section 210.123, RSMo, the relative shall have the authority to make the day-to-day decisions for the care of the child for the duration of the TAPA and shall further have the authority to make educational and medical decisions for the child. The relative shall consult with the child’s parent(s)/legal guardian(s), and the Children’s Division before making decisions pertaining to the child other than routine, day-to-day decisions necessary for caring for the child.
Pursuant to 13 CSR 35-30.030, staff will provide the relative with the Official Notice of Temporary Placement of a Child Form (CD-294) to notify schools, medical care providers and others that the relative has the temporary authority to make day-to-day decisions, educational decisions, and medical decisions for the child for the duration of the TAPA. The relative provider shall retain the original copy, but may provide copies for any individual or institution for their records as needed. Upon termination of the TAPA the relative shall notify each individual or institution who has received a CD-294 that the TAPA has terminated.
It is the responsibility of the relative to notify each individual and/or provider who was provided a copy of the CD-294 of the termination of the TAPA.
Pursuant to 13 CSR 35-30.030, the relative shall agree to the following during the implementation:
-
-
- Making the child available to meet with the Children’s Division in person, virtually or by other means of communication at least two times each month to enable staff to monitor the implementation of the TAPA and to ensure that the TAPA is being safely implemented. At least one visit each month shall be in the Relative’s home at the discretion of the Children’s Division, the other visit may be virtual or in the community;
- Allowing the Children’s Division to inspect the home of the Relative where the child resides, including allowing the Children’s Division to meet with the child, in-person in the home of the Relative at least one time a month, and the home of the Parent, at reasonable times (announced and unannounced) to monitor the implementation of the TAPA and ensure the child is safe and well cared for during the TAPA;
- Executing any consents and/or authorizations to release information to the Children’s Division and/or to or from third parties that the Children’s Division determines necessary for the Children’s Division to obtain information to develop and/or monitor implementation of the TAPA. This includes, but is not limited to health care providers, schools and school districts and other professionals providing services to the child and the parties to the TAPA;
- Participating in all TDMs that the Children’s Division may convene pertaining to the child;
- Keeping the Children’s Division informed of their current residence address, mailing address, telephone number, e-mail address, work address and contact information; and any change in the residence of and contact information for the child;
- Promptly notifying the Children’s Division of any change in circumstances that may impact the care of the child and/or the implementation of the TAPA;
- Providing full, truthful, accurate and complete information to the Children’s Division and other members of the TDM;
- Ensuring the child resides in the State of Missouri for the duration of the TAPA unless the child requires medical treatment in another state that is not reasonably available within the State of Missouri. The Child’s Parent and the Relative shall immediately notify the Children’s Division if the child requires medical care out of state; and
- Participating in the services the parties identify as necessary to the TAPA.
-
9.2.2.5 Team Decision Making (TDM) Meetings
When there is a Temporary Alternative Placement Agreement (TAPA) a Team Decision Making (TDM) Meeting is required. Pursuant to 13 CSR 35-30.030, a TDM means a group of individuals invited by the Children’s Division to form a team to assist, support, and advise the Children’s Division and the parties to the TAPA on making decisions involving the children and family with the goal of successfully implementing the TAPA.
Pursuant to 13 CSR 35-30.030, TDM meetings shall be informal, and shall be held at times and places that are reasonably convenient for as many of the participants as possible, with priority given to the schedules of the mandatory TDM members. TDM meetings may be held in person at the offices of the Children’s Division or at other mutually convenient locations. TDM meetings may also be held by conference call or other electronic means.
Composition of TDM Meetings
-
-
- Mandatory TDM Members: Pursuant to 13 CSR 35-30.030, the members of the team for a TDM shall include representatives of the Children’s Division, the child’s Parent, the Relative, the child’s guardian ad litem if the child has a guardian ad litem, any other party to the TAPA, and the attorney for any of the parties to the TAPA, at the request of that party. A TDM meeting may still be held if all of the mandatory team members are not in attendance.
-
-
-
- Optional TDM Members: Pursuant to 13 CSR 35-30.030, the team may also include other relatives of the children and parents as well as school personnel, Probation and Parole personnel, medical and mental health personnel, the juvenile officer if the juvenile officer requests to be present, service providers to the child and family, and any other individual who the parties to the TAPA agree may provide constructive advice, assistance and support for the implementation of the TAPA.
-
-
-
- Children’s Participation Pursuant to 13 CSR 35-30.030, children twelve (12) years of age and older should attend TDM Meetings, if the child is willing and able to attend the meetings, and Children’s Division believes their attendance is in the child’s best interests.
-
Pursuant to 13 CSR 35-30.030, the Children’s Division may exclude from any TDM meeting any person who is, or the Children’s Division has reasonable cause to believe may become, disruptive to the orderly management of the case and/or meeting. Staff may exclude from the TDM any non-mandatory team member who becomes disruptive to the meetings and successful implementation of the TAPA.
If the juvenile officer or guardian ad litem is not in attendance, Children’s Division will inform them following the TDM meeting of the decision(s) made.
Pursuant to 13 CSR 35-30.030, the failure of any party to a TAPA to attend and fully participate in TDM meetings in good faith may be grounds for the Children’s Division to take appropriate action including, but not limited to notifying the juvenile officer that the parties are not participating in the TAPA and/or terminating the TAPA.
An initial TDM Meeting is a facilitated meeting to review the threats to the child’s safety and to make a team decision around initial diversion placement decisions for the child. Whenever feasible, the initial TDM Meeting should be held prior to the diversion of the child in order to explore all options available to the family and to mitigate the safety threat(s). An agenda for initial TDM Meetings prior to a diversion may include:
-
-
-
- Diversion placement decisions related to safety of the child to include exploring a TAPA;
- Decisions whether the child can remain in the home with an Immediate Safety Intervention Plan (CD-263);
- A review of how the health, care, safety and welfare of the child is being assured;
- Any matters that any member of the TDM may wish to add to the agenda.
-
-
Pursuant to Section 210.123, RSMo and 13 CSR 35-30.030, initial TDM Meetings are to be held in situations where a child and parent have been separated through a TAPA and must be held within ten (10) days of the execution of a TAPA.
9.2.2.5.2 Facilitating TDM Meetings
Pursuant to 13 CSR 35-30.030, Children’s Division staff members will facilitate TDM Meetings, unless otherwise agreed between the parties to the TAPA. Based on the complexity of the case, a Children’s Service Worker, Children’s Service Supervisor, the assigned Family Centered Services (FCS) worker, or the assigned Alternative Care (AC) case manager can act in a third-party neutral facilitator role. A supervisor is not required to attend the TDM Meeting. Supervisors should attend TDMs with new workers until the worker demonstrates proficiency in the facilitation of the TDM.
In complex situations where a circuit identifies that a trained TDM facilitator is needed and they do not have a local TDM facilitator available, they may reach out to a regional team of TDM facilitators to facilitate the TDM Meeting. Complex TDM meetings should be considered on a case-by-case basis due to the unique circumstances that bring the family to require a TDM. Complex Situations for TDM may include, but are not limited to:
-
-
-
- Domestic violence situations, especially where separate meetings are necessary;
- When mental health or substance use issues present worries that the discussion will be difficult to keep calm and productive;
- Human Trafficking Cases;
- Child fatality cases where there are other siblings involved;
- Conflict reports (employee reports/external conflict reports);
- Cases involving custody disputes; and
- Juvenile officer is adamant to take custody (or not), and CD does not agree with the recommendation.
-
-
Pursuant to 13 CSR 35-30.030, staff should have a clear purpose and agenda planned for the TDM after the execution of the TAPA. The TDM agenda shall include:
-
-
-
- A review of how the health, care, safety, and welfare of the child is being assured;
- The progress so far in implementing the TAPA;
- A discussion of any challenges in implementing the TAPA and how challenges may be addressed;
- A discussion of what next steps are necessary to progress toward termination of the TAPA; and
- Any matters that any member of the TDM may wish to add to the agenda.
-
-
Pursuant to 13 CSR 35-30.030, decisions shall be made by consensus of the members of the TDM. No party to the TAPA or the Children’s Division is legally bound by any decision made at a TDM. All decisions shall be voluntary.
If no decision can be made, then the final decision should be determined by:
-
-
-
- Amending the TAPA and notifying the Juvenile Office of changes to the TAPA;
- Keeping the TAPA as agreed upon by all parties; or
- Terminating the TAPA and making a referral to the Juvenile Office by submitting a CD-235 with a recommendation for further action.
-
-
9.2.2.5.3 Documenting a TDM Meeting
Pursuant to 13 CSR 35-30.030, the Children’s Division shall maintain documentation of each TDM meeting. Any agreements reached during the TDM to revise the TAPA shall be reduced to writing and signed by all of the parties to the TAPA. The Children’s Division will provide the Juvenile Officer with a copy of the revised TAPA.
-
-
-
- During the TDM Meeting, staff should develop, review, and revise the TAPA with the family and participants of the meeting.
- Pursuant to 13 CSR 35-30.030, any agreements reached during the TDM to revise the TAPA shall be reduced to writing and signed by all of the parties to the TAPA. Staff will provide the juvenile officer with a copy of the revised TAPA. Summarize the notes and decisions of each TDM Meeting and provide copies of the summary to all participants.
- Document the TDM Meeting with a summary of the discussion and decisions in FACES using the contact communication log for the purpose of TDM.
-
-
9.2.2.6 TAPA Monitoring Requirements
A plan for monitoring the safety of the child must be developed in the Immediate Safety Intervention Plan (CD-263) and the Temporary Alternative Placement Agreement form (CD-295) as discussed elsewhere in this chapter.
To further assist in monitoring the safety of the child and the parent/legal guardian’s progress with the plan developed through the TAPA, the following must also occur:
-
-
- A Family Centered Services (FCS) case must be opened within ten (10) days of the execution of the TAPA, and the case must remain open during the duration of the agreement. Follow Child Welfare Manual – Section 3 – Delivery of Services/Intact Families FCS Policy for provision of FCS services with a TAPA;
- Staff must have personal contact with all the children on the TAPA as appropriate to ensure that the TAPA is being safely implemented, but no less than two (2) times per month. One (1) contact with each child must be a face-to-face observation of the child in the child’s relative diversion placement. Additional contacts with the child may occur virtually or in the community.
- At least one face-to-face home visit per month must be completed on all FCS cases with the parents involved in the TAPA.
- A Team Decision Making (TDM) Meeting must meet at least once every month thereafter for the duration of the TAPA.
- A review/update Safety Assessment must be completed within thirty (30) days or at the initial TDM meeting and every thirty (30) days at the ongoing TDM meetings thereafter until the TAPA is terminated.
-
Pursuant to 13 CSR 35-30.030, parties to the TAPA may ask the Children’s Division to schedule additional meetings.
The TAPA should address visitation between the child and the parent. Staff should be mindful of all custody arrangements that address visitation, as those should continue to be followed during the TAPA. If there is a safety concern inhibiting contact between the child and the parent or another barrier, the parents must agree to any adjustments to court-ordered visitation arrangements. Staff should not supervise visitation. If the parent and the relative cannot agree to a visitation plan, this means essentially they fail to come to an agreement on the diversion placement and the stipulations of a TAPA and staff should make a referral to the juvenile officer by submitting a CD-235. If supervised visitation is necessary, the parties should consider utilizing a third-party. Staff must complete background checks on all third party supervisors including: CA/N, case net, and sex offender registry checks as described elsewhere in this section.
9.2.2.8 Duration and Termination of the TAPA
Maximum Length of a TAPA
Pursuant to Section 210.123, RSMo, a TAPA shall be valid for no longer than ninety (90) days. If the goals of the TAPA cannot be accomplished within ninety (90) days and the child cannot yet be safely returned home, a referral to the juvenile officer must be made as soon as possible, but no later than ten (10) days prior to the end date of the TAPA by submitting a CD-235. In the referral, staff may recommend a second TAPA instead of recommending removal. Additional TAPAs should rarely be needed for another full ninety (90) days. For example, a second TAPA may be requested if the relative has begun the process to obtain guardianship, but the court date will not occur prior to the end of the first ninety (90) days.
If there is good cause to enter into a second TAPA beyond the first ninety (90) days, a TDM must be held prior to the ninety (90) day expiration. The TDM should discuss and document the reasons for a second TAPA and how long the second TAPA will be needed. Staff must obtain approval from the Regional Director, or their designee, for any additional TAPAs beyond one hundred twenty (120) days. The initial TAPA and the second TAPA cannot exceed a total of one hundred eighty (180) days.
Request to Terminate a TAPA
Except in emergency situations where removal of the child from a relative is beyond the control of the provider, the parent and/or relative may terminate the TAPA at any time. Pursuant to 13 CSR 35-30.030, this may be done by the party submitting five (5) days’ written notice. Pursuant to 13 CSR 35-30.030, parties to a TAPA are encouraged, but not required, to ask to schedule a TDM meeting before voluntarily terminating a TAPA to see if the team can help resolve any issues that may cause the party to consider withdrawing from the TAPA. Staff should hold a TDM to determine whether a new TAPA is needed and to address diversion placement issues. If a new TAPA cannot be negotiated, and the safety threat(s) still exist such that a diversion remains necessary, a referral to the juvenile officer should be made by submitting a CD-235 immediately upon receiving notice of the request for termination.
Pursuant to 13 CSR 35-30.030, if the relative is no longer able to care for the child due to an emergency, the relative will notify the Children’s Division immediately. The remaining parties to the TAPA will confer to determine whether a new TAPA is appropriate and, if so, then the parties will implement a new TAPA. The Children’s Division must schedule an emergency TDM meeting to facilitate the meeting between the remaining parties to the TAPA.
Completion of a TAPA
Pursuant to 13 CSR 35-30.030, the TAPA expires five (5) days after successful completion of the plan set forth in the TAPA, provided that the Children’s Division shall be given sufficient time to complete and submit the Notification of TAPA Termination (CD-298) to the juvenile officer. If there is no longer a need for a TAPA because the safety threat(s) have been eliminated and the child can safely return home, staff must submit a written report to the juvenile officer no later than ten (10) days prior to the termination of the TAPA. Staff should utilize the Notification of TAPA Termination (CD-298) form as the final report to the juvenile officer. Pursuant to Section 210.123, RSMo, a copy of the CD-298 shall also be given to the parent/legal guardian and the relative. Staff must upload the completed CD-298 to OnBase.
The child may return home prior to submitting the CD-298; however, staff must send the report as soon as possible and no later than ten (10) days prior to the original date of TAPA expiration.
Pursuant to 13 CSR 35-30.030, a TDM may be held before the TAPA is scheduled to expire to discuss the successes and challenges of implementing the TAPA, whether a new TAPA may be necessary and to discuss whether any next steps may be appropriate.
A TAPA and the Children’s Division’s involvement may terminate if the safety of the child can be assured long-term as a result of the relative obtaining legal guardianship, legal custody of the child, or an entry of an order of child protection. For orders of child protection, staff should ensure a permanent, not just a temporary, order has been granted prior to case closure.
If the relative obtains (1) a power of attorney under Section 475.602, RSMo, or (2) an affidavit for a relative caretaker under Section 431.058, RSMo, the TAPA may be terminated. However, because these can be revoked by the parent at any time, staff may not terminate the Children’s Division’s involvement without first staffing the case with the supervisor and Circuit Manager or upon the recommendation of a TDM meeting, and a Family Safety Planning Document (CD-267) should be completed. If the relative obtains either a power of attorney or an affidavit for a relative caretaker within three (3) business days of the beginning of the diversion placement, a TAPA is not needed, and staff should utilize the Immediate Safety Intervention Plan (CD-263) to develop a plan to mitigate the safety threat(s).
9.2.2.9 Intensive In-Home Services (IIS) Referrals
If it has been determined that the child cannot safely remain in the home at the current time, but with IIS, the child could safely return home, an Immediate Safety Intervention Plan (CD-263) must be developed with the family. If IIS services are determined to be an effective intervention to ensure child safety in the home, the child may return home when IIS services are accepted and initiated in the home. Should IIS services not be implemented within three (3) business days of initiating a diversion placement, and conditions continue to warrant placement outside the home, a TAPA (CD-295) must be developed, or a referral to the juvenile officer must be made by submitting a CD-235 if the child remains in imminent danger. If IIS services are later implemented in the home and the child is safely returned, the TAPA can then be terminated.
9.2.2.10 Notifying, Referring, and Reporting to the Juvenile Officer
The Children’s Division retains the authority to refer the case to the juvenile officer with a recommendation for further action while a TAPA is in place. If at any time during the TAPA it is determined the goals are not being accomplished within the time period specified, and the safety, best interest, and welfare of the child cannot be assured if returned home, staff should refer the family to the juvenile officer.
To clarify from the sections above, pursuant to Section 210.123, RSMo staff must either notify, refer, or report the family to the juvenile officer at the prescribed and non-negotiable timeframes or in the following situations:
-
-
- If at any time staff determine a child is in imminent danger and no suitable short-term plan can be developed to mitigate the safety threat(s) a referral to the juvenile officer should be made by submitting a CD-235 immediately;
-
-
-
- If either the parent, the relative, and/or the Children’s Division are unable to come to a consensus on the negotiation of a TAPA, a referral to the juvenile officer must be made by submitting a CD-235 as soon as possible, but no later than three (3) business days from the beginning of the diversion placement;
-
-
-
- At the start of the TAPA, staff must notify the juvenile officer by sending the TAPA (CD-295) form. This notice must be provided no later than three (3) business days from the beginning of the diversion placement;
-
-
-
- If the parent/relative requests termination of the TAPA and the child cannot safely return home, a referral to the juvenile officer must be made by submitting a CD-235 as soon as possible. Staff should first consider convening a TDM to attempt to develop a new plan;
-
-
-
- Upon successful completion of the TAPA and the child’s return home, a report to the juvenile officer must be made by sending the Notification of TAPA Termination (CD-298) form as soon as possible or no later than ten (10) days before the date the TAPA was set to expire–whichever occurs first;
-
-
-
- If the goals of the TAPA cannot be accomplished within ninety (90) days and the child cannot yet be safely returned home a referral to the juvenile officer must be made by submitting a CD-235 prior to the end date of the TAPA.
-
All referrals to the juvenile officer are to be completed utilizing the JO Referral screen in FACES and submitting the CD-235 to the juvenile officer. Referrals do not require a recommendation for protective custody. The referral must include the Children’s Division’s recommendations regarding the care, safety, and placement of the child and the reasons for those recommendations. Recommendations may include:
-
-
- Recommendation to immediately remove the child prior to notice and hearing to the parents when there is specific, articulable evidence to indicate that the child is in imminent danger of serious bodily injury, death or sexual abuse;
- Recommendation to remove a child when there is specific, articulable evidence to indicate that the child is in danger of serious bodily injury, death or sexual abuse – but it appears to CD that there is time to submit the issue to the court for review; or
- Recommendation to remove a child, or to leave the child in the home/diversion placement under supervision, after notice to the parents and opportunity for a hearing before the court; or
- Recommendation to file a petition, but to leave the child in the home under judicial supervision under supervision of the Children’s Division.
-
9.2.2.10.1 When the Juvenile Officer Declines a Children’s Division Referral (CD-235)
Pursuant to the standards for the Juvenile Officer in matters of child abuse/neglect, all referrals to the Juvenile Officer must be made in writing, by utilizing the CD-235, and must be signed by the person making the referral. The juvenile officer shall make an initial and prompt determination regarding the sufficiency of the referral and determine whether:
-
-
-
- The jurisdictional elements are established in the referral;
- The referral contains a clear statement of the act alleged;
- There is sufficient evidence to support action by the Juvenile Officer; and
- The information supports the need for action by the Juvenile Officer.
-
-
The Juvenile Officer shall make a written request of the referring party for additional investigation or information necessary to determine the sufficiency of the allegations in the referral and include a reasonable period for response by the referring party or person. The Juvenile Officer shall provide, in writing, to the referring party or person the reason the referral is not sufficient to establish jurisdiction or warrant action by the Juvenile Officer.
Based on the response from the juvenile officer, staff should request a consult with the Juvenile Officer to discuss the reason a referral was rejected to ensure the Children’s Division’s concerns for the child’s safety have been clearly articulated. This consult should include the worker, supervisor, and Circuit Manager. Staff may need to provide or gather additional information to the Juvenile Officer.
If, after attempting to resolve the concerns of the Juvenile Officer around the sufficiency of the referral and the evidence available, the Juvenile Officer does not take further action, and the safety threat(s) to the child remain without further court intervention, the case must be staffed with a supervisor or higher-level manager to determine the most appropriate next steps. The Children’s Division should clearly document the reasons the Juvenile Officer rejected the referral in the case record.
9.2.2.11 Completing the TAPA (CD-295)
Parties Involved with a TAPA Agreement
A TAPA requires the full agreement of the parent(s)/guardian(s), relative(s), and the Children’s Division in order for the TAPA to be implemented. As such, contact information for the child, parent(s)/guardian(s), and relative(s) must be fully included on the TAPA form.
What immediate safety threat(s) to the child(ren) exist?
A safety threat is defined as a behavior, emotion, motive, perception, or capacity of a person who has access to the child that is out of control, imminent, and likely to have severe effects on a vulnerable child. When identifying safety threat(s), they need to be child-specific. Safety threats to a child are evident when a child is vulnerable to a particular situation and the parent/legal guardian does not have protective capacities to resolve the threat.
What are the child(ren)’s vulnerabilities to the safety threats and what are the concerns with the parent/caretaker’s protective capacities?
Vulnerabilities of a child are a significant factor in evaluating the safety and imminence of the identified safety threat(s). Child vulnerabilities are the degree to which a child is susceptible to threats to his or her safety and the degree to which a child is capable of protecting him/herself against those threats. Things that contribute to child vulnerabilities are age, developmental level and mental capacities, physical disabilities and illness, behaviors, ability to communicate, isolation/visibility, ability to meet basic needs, access to perpetrator(s), and the child’s relationship to the perpetrator(s).
The protective capacities of a parent/legal guardian are another vital element to consider when evaluating safety. Caregiver protective capacities are personal, behavioral, cognitive and emotional characteristics that are directly associated with child protection. There are several things that can impact the protective capacities of a parent/legal guardian, including mental capabilities, physical health, access to resources, relationship to the perpetrator(s), behavioral history, age, and substance misuse.
What actions has the parent/legal guardian taken in the past to keep the child safe when the safety threat(s) have occurred? What supports have been utilized in the past (or presently) to keep the child safe?
By exploring previous safety threats and what the parent/legal guardian did in the past to keep the child safe, strengths within the family are identified. Similarly, once past and/or present supports to keep the child safe are explored, possible support networks (either formal or informal supports) are identified that can assist with the current TAPA (CD-295). By expanding on strengths within the parental protective capacities and identifying natural supports within each family, staff are more easily able to assist the family in developing realistic plans that are specific to their family, making follow-through more likely. It also allows the parent/legal guardian an opportunity to feel actively involved in the plans for their family, instead of being directed on what to do from an outside agency.
Facts and Circumstances that Led to the Implementation of the TAPA
In this section of the TAPA form (CD-295), staff will identify the facts and circumstances of alleged abuse/neglect that led to the implementation of the TAPA, including:
-
-
- CA/N incident numbers that led to the Children’s Division’s current involvement with the family;
- Specific allegations and existing safety threat(s) to each child named in the TAPA and who/what poses the threat(s);
- How the parent’s protective capacities are insufficient to protect the child from the safety threat(s) and describe what makes the child vulnerable to the threat(s);
- Factual documentation from any relevant service providers/collateral contacts that contribute to the concern for child safety; and
- Actions taken thus far, and by whom, to ensure the immediate safety of the child involved in the TAPA
-
What needs to happen for this TAPA to successfully end and the child to safely return to the parent(s)/legal guardian(s)?
Staff should identify the action steps needed, and by whom, to resolve each identified safety threat(s) to each child named in the TAPA form. Each action step/plan shall include timeframes for completion as well as the behavioral changes that are needed to be made by each parent/legal guardian in order to ensure each child’s safety, best interest, and welfare upon returning home. When identifying specific steps that need to happen for the TAPA to successfully terminate, staff should be sure not to be heavily reliant on services, but rather on the behavioral changes needed to ensure safety. For example, the plan should not simply identify that a parent should participate in parenting classes. Instead, the plan should describe the behavior the parent needs to demonstrate in order for the Children’s Division to be assured the parent has developed sufficient protective capacities to protect the child from the safety threat(s). In this scenario, the parenting class is simply a resource the parent may utilize to help them be able demonstrate the desired behavior. It is not the parenting class itself that will keep the child safe, but the parents’ behavior as a result of attending the parenting class.
Similar to completing an Immediate Safety Intervention Plan, the TAPA should:
-
-
- Be realistic and time-limited;
- Ensure the parent(s)/guardian(s) and relative(s) are in agreement with the TAPA plan;
- Utilize the family’s own resources by focusing on existing strengths and natural family support network;
- Assess the reliability of resources and providers of the action/steps;
- Develop interventions to accommodate time elements (for example, weekends and holidays may require different actions than daytime hours during the week, etc.);
- Take into consideration the tradeoffs the family may have to make in order to successfully terminate a TAPA; and
- Be conscious to not create further trauma to the family/child
-
What safety-related resources/support services are currently in place or still need to be referred to assist with the behavioral changes needed to resolve the threat(s) of safety to the child? What services will the Children’s Division offer to the family? What supports have been utilized in the past that can be utilized during the TAPA to eliminate the safety threat(s)?
This section of the CD-295 is separated from the actual plan for safety, as a TAPA should not be reliant on services to make immediate behavioral change.
In this section of the CD-295, staff shall identify all safety-related services, service providers, and specific resources being offered to any and all parties involved in the CD-295, as well as what safety-related services and supports the family still needs to be connected with in an effort to prevent the removal of the child. These can be direct services provided by the Children’s Division, as well as any other services from community agencies that have been offered to the family to assist with the success of the TAPA and to reduce the risk of future CA/N. Safety-related services are appropriate services that are provided to or arranged for the family with the goal of ensuring child safety. For example, if there are safety concerns related to the parent’s ability to manage child-specific needs, Intensive In-Home Services (IIS) can be an appropriate safety-related service.
Staff should be sure to include timeframes for each service/resource and how the implementation of such service(s)/resource(s) will assist with the successful termination of the CD-295.
When staff determine safety-related services are needed during a CA/N report staff should clearly articulate and document the safety concern to include areas of need such as, but not limited to: basic needs, living conditions, the family’s support system, health, mental health, educational concerns, and help address the needs through community resources and/or the family’s safety network.
What is the plan for visitation and contact for each parent and all child(ren) with the participation of all parties?
In this section of the TAPA form (CD-295), staff should develop a visitation plan for each parent and each child. The visitation plan should be agreed upon by all parties of the TAPA and made in the best interest of the child and/or sibling group. The visitation plan is meant to enhance and increase the bond between the parent, child, and siblings for the duration of the TAPA. These standards should be considered by the parties when developing and reviewing the visitation plan.
Whenever possible, visits should occur in the parental home or in a homelike environment. This may include the home of the relative. Opportunities should be provided to allow the parents to participate in their child’s normal day-to-day activities, when possible. For example, a parent could attend parent-teacher conferences, extracurricular activities, and doctor or dentist appointments.
What steps should the family and/or safety network members take in the event this TAPA is violated? Provide the name(s) and contact information for all members of the family support network as well as all individuals who must be immediately notified if this TAPA is violated or there are concerns for the safety of the child(ren) involved in this plan.
The TAPA (CD-295) must include an action step(s) for notification if the plan is violated or concerns arise regarding the safety of the child. This action step(s) should be developed so that all those involved in the TAPA (including formal/informal family supports, collaborative team members, service providers, etc.) will know what to do in the event the plan is violated. This should include contact information for all those who must be immediately notified if the plan is violated or concerns arise regarding the safety of the child.
Once the CD-295 is developed, the worker should make sure the family and any safety network members actively involved in the plan have a copy. The worker can take a picture of the plan for the record and provide the family with a paper copy. A copy must be retained and uploaded to OnBase.
By agreeing to this TAPA, parent(s)/legal guardian(s) agree and understand the following:
Staff must explain all the legal requirements for entering into a TAPA and have the parent(s) or legal guardian(s) and the relative(s) initial their respective sections on the TAPA form (CD-295).
The parent/caretaker must be given a choice to participate in the safety planning process. There may be times when families refuse to enter into an Immediate Safety Intervention Plan. If so, they must be made aware of the potential consequences if staff feel the child’s safety cannot be assured. Staff may need to consult with their supervisor and/or make a referral to their law enforcement or juvenile office if a family refuses to enter into an Immediate Safety Intervention Plan.
Staff must refrain from the use of ultimatums or any other similar practices. The use of ultimatums is a direct contradiction to strength-based, family-centered practice, and may be construed as an oppressive act of coercion. Staff may inform families of possible actions, such as a report being filed with the local juvenile court, which may take place should children’s safety or wellbeing continue to be a concern beyond the Division’s ability to enter into a voluntary safety agreement with all suitable relatives or kin, including non-resident parents. However, staff may not tell a family that failure to enter into a specific safety plan, especially one that the family is not in agreement with, will result in their child(ren) being removed from their custody. Staff should consult their supervisory channels as needed when facing situations of unresolved children’s safety or wellbeing.
The Family Safety Planning Document (CD-267) is to be used to guide your conversations with the family and their network to develop the plan that will enable them to achieve and maintain the safety goal(s) for their children.
The CD-267 should be used once a safety goal has been developed with the family. The CD-267 creates the road map for how the safety goal will be achieved. Developing the Family Safety Plan will often take time and must be created primarily by the family and their network. If there is a need to address immediate safety concerns, staff should use the Immediate Safety Intervention Plan (CD-263).
The danger statement and safety goal must be developed prior to starting the CD-267. The danger statement is necessary so everyone is clear about the worries for the children and their families. Having clearly established safety goals will ensure that everyone comes to the safety planning endeavor with a common vision of the desired outcome the plan is meant to achieve. The CD-267 should be developed with a focus on how people will be living differently to help keep the children safe now and in the future, even after the Children’s Division’s case is closed.
The CD-267 should NOT focus on services that will be provided to families. Instead, the CD-267 guides the development of a specific set of rules and arrangements that describe how the family and network will show everyone that the child(ren) will be safe in the future. As the case progresses, it is expected that the CD-267 will be modified and refined.
A safety network should always be involved in the creation, implementation and monitoring of the Family Safety Plan (CD-267).
9.4.1 Components of the Family Safety Planning Document (CD-267)
Signs Things are Going Well: What does it look like when things are going well, related to the worries?
Triggers: Circumstances, conditions, or situations that have caused or might cause the worries to start or be worse.
Preventative Plan: Steps people will take to keep the good things happening and/or to prevent the worrisome behaviors from starting (steps to manage the triggers).
Red Flags/Warning Signs: Things that tell everyone the response plan should be used right away.
Response Plan: Steps the family and/or the safety network will take to keep the kids safe when the warning signs are first noticed.
The details for each component of the Family Safety Plan are often captured during Three Column Conversations and then transferred to the Family Safety Planning Document (CD-267).
|
What are we worried about? |
What’s working well? |
What needs to happen? |
|
Triggers? What has triggered the worrisome behavior in the past? What could trigger the worrisome behavior in the future? **Tells the safety network to be on high alert and to use the Prevention Plan.
Red Flags? What are the first signs that the worrisome behavior is about to happen? **Tells everyone to activate the response plan.
|
Signs things are Going Well? How can you tell when the worries are not present or that the goals are being met even in small ways?
Prevention Plan Ideas What has kept or is keeping the worries from starting?
Response Plan Ideas How have the kids been kept safe in the midst of the worries?
|
Prevention Plan Rules What else will be done by whom to keep the worries from starting?
Response Plan Rules What else will be done by whom to keep the kids safe in the midst of the worries?
**Establish agreements about who will do what else, when, to protect the kids in the future. |
9.4.2 Monitoring the Family Safety Plan (CD-267)
As the CD-267 is utilized, it must be constantly evaluated, monitored, and adjusted as necessary. Families should be given opportunities to incrementally demonstrate how they are using their plan as the case progresses. As the use and effectiveness of the plan are demonstrated, contact with the children should gradually increase and become less restrictive.
Some ways the CD-267 can be monitored may include:
-
- Unannounced home visits by Children’s Division staff or safety network to observe how the CD-267 is being used;
- Have Three Columns Conversations with parents, children and network members to understand and compare their perspectives on how the plan is working;
- Have the family keep a safety journal where they can write their comments about how the CD-267 plan is working;
- Safety network meetings to review progress and assess the level of confidence in the safety plan based on how it is working;
- Rehearse, test, and/or practice different parts of the CD-267. As the CD-267 is developed, each revision should be shared with the family and the safety network. A child’s version of the CD-267 plan should be created so the child(ren) can understand what will be done by whom to keep them safe. Tools such as the Words and Pictures or the My Safety House (CD-216) are useful for turning the CD-267 plan into a child-friendly version. Any significant revisions of the CD-267 may indicate a need to update the child(ren)’s version of the safety plan.
Bottom lines are really less about the power differential and more about non-negotiable parts of the process. For example, involving a safety network and creating an age-appropriate explanation for the children are two of the most common process bottom lines. Occasionally, but not often, the Children’s Division will have bottom lines about the details of the Immediate Safety Intervention Plan or TAPA. For example, in a child sexual abuse case, the agency will almost always set a bottom line that the alleged offender can never be alone with the children.
Total equality between the professionals and the family can never be achieved. Families often ask if their children are going to be taken away. That is because they view staff as having power and authority over them. Children’s Division staff should recognize that they are in positions of authority and should be sensitive to how this is managed. Due to the Children’s Division’s statutory obligation to protect children, decisions frequently have to be made that will have negative consequences for families. Staff should be open and honest about the agency’s bottom lines– the decisions the agency will have to make if the family is unable to make a plan that ensures the safety of their children. When families understand the bottom lines, they are better able to make fully informed decisions about how they are going to address the concerns of the professionals involved.
9.6 Responding to Youth Presenting Signs of Suicide
Assuring child safety extends beyond mitigating threats imposed by others, but also includes recognizing and responding to youth presenting suicidal behavior. When staff observe signs of suicide, or when a youth makes a plea for help, staff shall take steps to ensure the youth’s safety by immediately engaging appropriate mental health professionals. There should be a deliberate transfer of intervention from staff to the mental health professionals trained to assess and manage the crisis. This may include the youth’s therapist, if applicable and available, or it may involve contacting a crisis line for direction.
- Contact 9-1-1 if the youth has made a suicide attempt, or has verbalized suicide plans and has ready access to lethal means.
If this is not the case:
- If the youth is already working with a mental health professional – a therapist, or a community behavioral health center worker – staff should make contact with this individual first due to the existing professional relationship.
- If contact is made, staff shall follow the guidance provided by the mental health professional.
- If the youth does not have a current working relationship with a therapist or community behavioral health center worker – or they are unavailable at the point of attempted contact – staff shall contact:
- Access Crisis Intervention (ACI) Hotline, see Missouri Department of Mental Health’s Suicide Prevention page. A statewide, 24-hour crisis line that provides assistance or appropriate intervention, performing a mental health screening to render a clinical disposition for next steps, or
- Suicide Prevention Lifeline, 1-800-273-TALK (8255): A national 24-hour hotline for individuals experiencing a suicidal crisis or emotional distress.
The youth must not be left alone until contact is made with a mental health professional and guidance received for next steps. Until further guidance is received from a mental health professional, staff must ensure a plan for immediate and constant supervision. The discussion and plans made with the family to address safety issues must be clearly documented in a contact note within the FACES case record.
Related Practice Points and Memos:
07/27/2023 – PA23-IA-02 – Juvenile Assessment Safety Planning