
(Effective 04/15/19)
Table of Contents
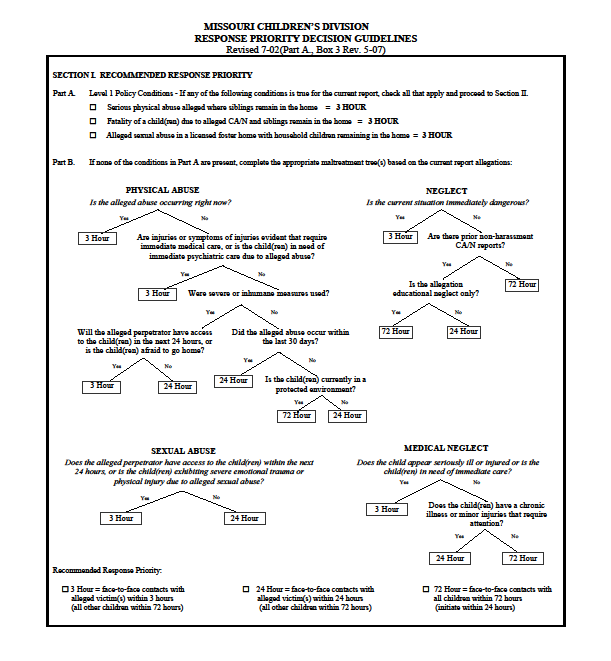
2.2.1 Response Priority Levels
2.2.1.1 Criteria for Level One Response Priority
CANHU uses the Structured Decision Making (SDM) tool below to determine the appropriate response priority for all CA/N reports. Response time begins at the time that the call is made. Call time can be found in FACES on the CA/N Report and Referral Status Log and the New Call Information Worksheet.
2.2.1 Response Priority Levels
There are three response levels, which are applicable for Investigations, Family Assessments, and Juvenile Assessments:
Level 1 – This is equivalent to an emergency report. Face-to-face contact with all victim(s) must be made within three (3) hours from the receipt of the report. A face-to-face contact by the Children’s Division with all children living in the household (victims and non-victims) must be made within 72 hours. Available resources shall be utilized to locate the child(ren), including law enforcement assistance.
Level 2 – Face-to-face contact with all victim(s) must be made within 24 hours from receipt of the report. A face-to-face contact by the Children’s Division with all children residing in the home (victims and non-victims) must occur within 72 hours.
Level 3 – Face-to-face contact by the Children’s Division with all children residing in the household (victims and non-victims) must be made within 72 hours from receipt of the report. NOTE: Because the law requires all CA/N reports to be initiated within 24 hours, Children’s Division staff should not wait longer than 24 hours to start working the report, even if they do not make face-to-face contact with the children until after that timeframe for a 72 hour report, unless the only basis for the report is educational neglect, which then must be initiated within 72 hours.
In situations where CD field staff have directly observed a home (or other situation) before calling the hotline, CANHU staff will defer to the field worker’s professional judgment if the worker has determined that the situation warrants an emergency:
- If the SDM Response Priority decision is not an emergency, CANHU will override to an emergency (within 3 hours) response based on the field staff’s direct knowledge of the situation. CANHU will document in the narrative that this report was upgraded from a lower SDM priority response to an emergency based on field staff’s direct knowledge of the situation.
- CANHU will not downgrade a call that has been screened as an emergency at the time of the call. Downgrading priority response levels may occur at the county office level, given additional information according to policy. Refer to Section 2, Chapter 3.4, Response Priority Level Override.
2.2.1.1 Criteria for Level One Response Priority
The following list includes examples of information received by the Child Abuse/Neglect Hotline Unit (CANHU), which would result in a CA/N report being assigned a Level One Response Priority:
- All reports of physical abuse occurring at the time of the report.
- All reports of serious physical abuse with household children remaining in the home and in danger of immediate harm.
- Reports alleging sexual abuse in a licensed foster home with any child remaining in the household, including children not in Division custody.
- All reports of severe physical injury where abuse or neglect is suspected to have occurred; immediate medical and/or social service attention is indicated and where the child is unprotected.
- All reports of sexual abuse where the alleged perpetrator continues to have unsupervised access to the child, there is a reported physical injury as a result of sexual abuse, the child is, at the time of the report, experiencing severe emotional trauma.
- Reports involving children who are, at the time of the report suffering from serious, untreated medical conditions which require immediate attention. This shall include all situations involving suspected or known instances of withholding of medically indicated treatment from infants with disabilities who have life-threatening conditions. (These situations are referred to as “Baby Doe” cases).
- Reports alleging that parents/caretakers of children are, at the time of the report, or within the preceding 24 hours, behaving in a bizarre manner or acting under the influence of drugs or alcohol and that they could pose an immediate danger to the children.
- Reports that children have ingested or been given drugs or alcohol, at the time of the report or within the preceding 24 hours, and because of their age and other concerns may be at immediate risk.
- Reports alleging children are presently being threatened with a dangerous weapon by a parent/caretaker.
- Reports alleging bizarre punishment are, at the time of the report, being administered to a child (i.e., locking a child in a closet, tying a child to a bed)
- Reports alleging that children are suicidal and appear to be, at the time of the report, contemplating suicide because of abuse or neglect.
- Reports alleging children have, at the time of the report, been left unsupervised, their parents whereabouts are unknown and because of their age or other concerns may be in physical danger.
- Reports from hospitals stating that a child, who is presently in their facility, is being released, may be in physical danger, and the hospital is unwilling to take protective custody.
- All reports involving exposure where, at the time of the report, a child is experiencing exposure to extreme weather conditions (i.e., heat, cold).
- Report of the death of a child where abuse or neglect is suspected and siblings remain in the home.
- Reports alleging that there is an active methamphetamine laboratory in a home that includes a child.
- Self-Referrals from parents who state they feel they will hurt or kill their child; request immediate removal of the child; or state they will immediately abandon their child. If a parent is requesting immediate placement of the child solely because the child is in need of mental health services that the parent cannot access or afford, a Preventive Service referral is to be taken according to the Voluntary Placement Agreement policy (VPA).